Impact
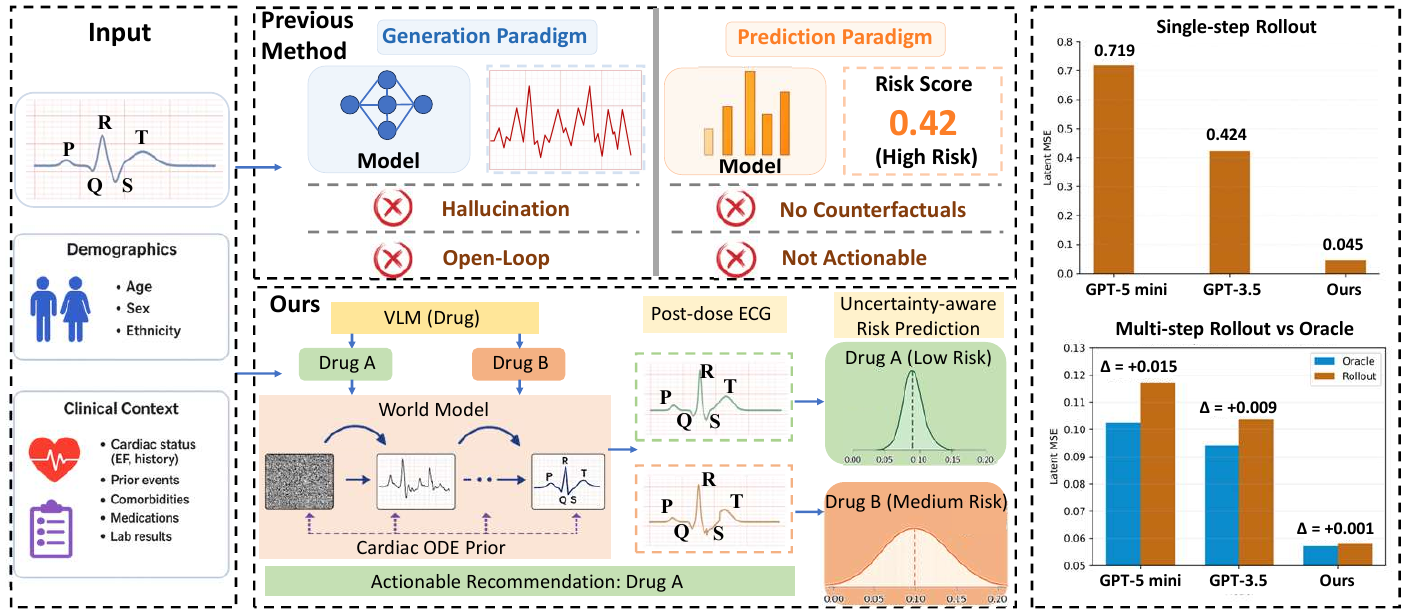
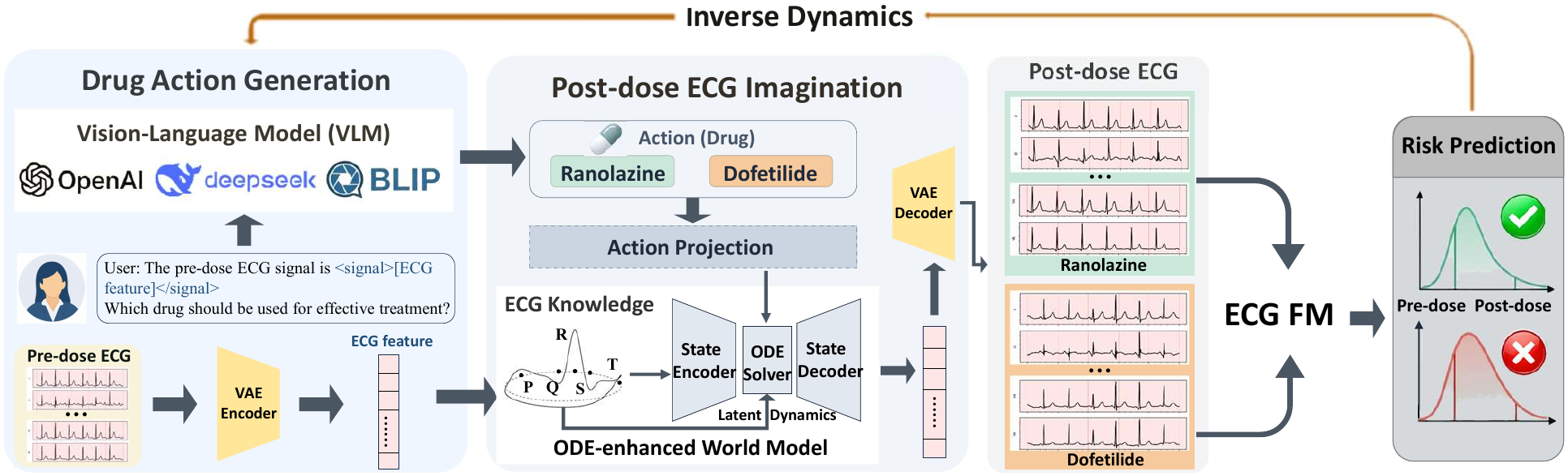
This work proposes an ECG World Model for simulation-based analysis of cardiac
interventions, enabling AI systems to explore potential physiological responses
under different treatment scenarios. By combining a physiological prior with
data-driven generative modeling, the framework supports hypothesis generation
and in-silico evaluation of treatment effects.
Limitations
-
Data Coverage. The model is trained on observational and
simulated data, which may not fully capture real-world complexity, variability,
or rare edge cases. This can lead to deviations from true clinical outcomes
under distributional shifts.
-
Simplified Prior. The physiological prior is simplified and
may be misspecified, limiting its ability to represent full cardiac dynamics,
especially in pathological regimes.
-
Evaluation Scope. Evaluation focuses on aggregate stability
metrics rather than clinical endpoints, and does not fully explain the interaction
between prior-driven and data-driven components.
-
Safety Guarantees. The model lacks calibrated uncertainty
estimates and formal safety guarantees, constraining its use in high-stakes settings.
Important. This system is not intended as a
standalone clinical tool. It should be used only as a decision-support framework
requiring expert validation. Generated scenarios should be treated as exploratory
hypotheses rather than definitive predictions.
Despite these limitations, the model exhibits stable and bounded behavior across
varying levels of prior mismatch, with variability increasing smoothly rather than
collapsing. The influence of the prior is also continuous and controllable, as
partial prior injection yields intermediate performance. These results suggest a
degree of robustness under imperfect assumptions.
Overall, this work takes a step toward more robust and interpretable generative
models for physiological simulation, while underscoring the need for further
validation, mechanistic understanding, and safety-aware design prior to real-world
deployment.